

Background: Historical treatment guidelines for the myeloproliferative neoplasm, polycythemia vera (PV), have generally not recommended cytoreductive therapy for "low risk" PV (age <60 and no prior thrombo-hemorrhagic events (TH)) on the hypothesis that decreasing the risk of TH events is the only goal of therapy for PV. The MPN-QOL Study Group has previously reported on the presence of PV associated symptoms, sometime severe, in PV including "low risk" PV patients. Recently, data from the ongoing "Low PV" interventional trial of RoPEG Interferon (INF) vs. Phlebotomy alone suggests an advantage in symptom control and event free survival in "low risk" PV patients treated on the RoPEG INF cytoreductive arm (LBA EHA 2020). Given this latter trial might alter the approach to managing "low risk" PV patients we sought to assess the symptom burden (with or without cytoreductive treatments) in that population.
Methods: MPN patient data was collected prospectively amongst an international cohort of PV patients including symptom burden, demographics, and disease features collected by IRB approved de-identified survey questionnaires (N=2,017, of which 698 had PV). We analyzed data from a subgroup consistent with "low risk PV" (age <60, no prior thrombo-hemorrhagic events). All participants completed the MPN-specific symptom burden questionnaire (MPN-SAF TSS [MPN-10]) and had no prior history of splenectomy. Surveyed symptoms on the MPN-10 included the patient's perceptions of common MPN-related symptoms and overall quality of life (QOL) on a 0 (absent) to 10 (worst imaginable) scale.
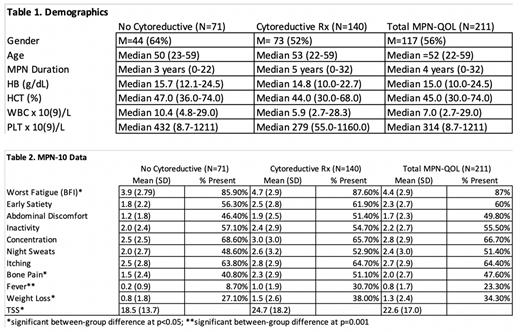
Results: A total of 211 "low risk" PV patients were identified, of which 140 (66.4%) had received some form of cytoreductive therapy (hydroxyurea = 54%; pegylated interferon = 44%; and anagrelide = 2%), with those patients not on cytoreductive therapy being statistically significantly younger (M=48.2±8.74 years vs. M=50.6±7.41 years), having a shorter duration of an MPN diagnosis (M=4.6±4.82 years vs. M=6.7±6.00 years), and higher hemoglobin (M=16.9±3.26 vs. M=15.2±2.37), higher hematocrit (M=50.6±9.83 vs. M=45.5±7.10), higher leukocyte (M=10.8±4.25 vs. M=7.5±4.72), and higher platelet counts (M=508.1±317.19 vs. M=327.8±190.52) at the time of MPN symptom assessment (Table 1). The entire cohort was quite symptomatic with 87% (n=184/211) of patients endorsing fatigue, but overall the PV patients on cytoreduction were more symptomatic (mean MPN-10 of 24.7 (cytoreduction) vs 18.5 (no cytoreduction) p=0.01) with significantly higher levels of fatigue (p=0.04), bone pain (p=0.04), fever (p=0.001) and weight loss (p=0.04) in cytoreductive group (Table 2).
Conclusions: "Low risk" PV patients are frequently symptomatic, and an unselected series from the MPN-QOL Study Group demonstrates significant symptomatic unmet needs in this population potentially supporting the need and potential benefit of cytoreductive therapy. "Low risk" PV patients (even before the impact of the Low PV Study is realized) also have frequently been receiving cytoreductive therapies, even though they have not been included in treatment guidelines, and typically have higher symptom burden despite lower counts, are older, and have longer duration of MPNs. Drivers of the decision to use cytoreductive therapy was not captured, but it is possible longer duration of disease, higher symptom burden, intolerance of phlebotomy might all be contributing factors. These results show there is both unmet need, and frequent heterogeneity amongst "low risk" PV patients, the final results of the Low PV Study are anticipated with great interest.
Mesa:Novartis: Consultancy; LaJolla Pharmaceutical Company: Consultancy; Samus Therapeutics: Research Funding; Sierra Oncology: Consultancy; Genentech: Research Funding; Incyte: Research Funding; AbbVie: Research Funding; CTI BioPharma: Research Funding; Promedior: Research Funding; Bristol Myers Squibb: Research Funding. Barbui:Italfarmaco: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees; AOP: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal